Gastric Stasis in Rabbits
Gastric stasis is one of the most common medical problems seen with small herbivores. Like many other common medical issues, it’s not a single issue, but a set of clinical signs that can have a variety of underlying problems. Think of stasis in the same way as thinking of colic in a horse or like “herbivore ADR.” This analogy explains why some algorithms exist that show how to treat it symptomatically, but also emphasizes the need for some diagnostic testing to rule out different diagnoses in order to provide the best treatment options. But what causes GI stasis? What testing should be offered? When does an animal need inpatient care? These are some of common questions that I get when I am called for consultations.
What causes stasis?
The first step in deciding on a diagnostic and treatment plan is understanding the underlying pathophysiology. The trick here is that due to the great number of underlying issues, the pathophysiology is vast. Some are acute, some more insidious. Most are GI related, but not all:
Dental disease is rampant in rabbits and common in guinea pigs and chinchillas. Rabbit teeth grow 2-4 mm per week. By comparison, horse teeth grow that same amount in a year. As sharp points develop on the lingual aspect of the teeth, the hay intake is reduced in favor for easier to chew pellets and vegetables. This reduces fiber intake, and fiber is a key stimulant for normal motility.
During periods of heavy shedding, a great deal of fur may be ingested during the grooming process. There is always a normal fiber mat in the stomach. The ingested fur and fiber can pass through the pylorus in a large ball and create an obstruction in the proximal intestine.
Bladder stones may cause low level discomfort that becomes an acute problem when it moves in and out of the outflow of the bladder. The pain can inhibit motility and reduce the food drive. I have seen bad corneal ulcers do the same.
Lop eared rabbits are predisposed to liver lobe torsion that will cause very sudden and very severe pain.
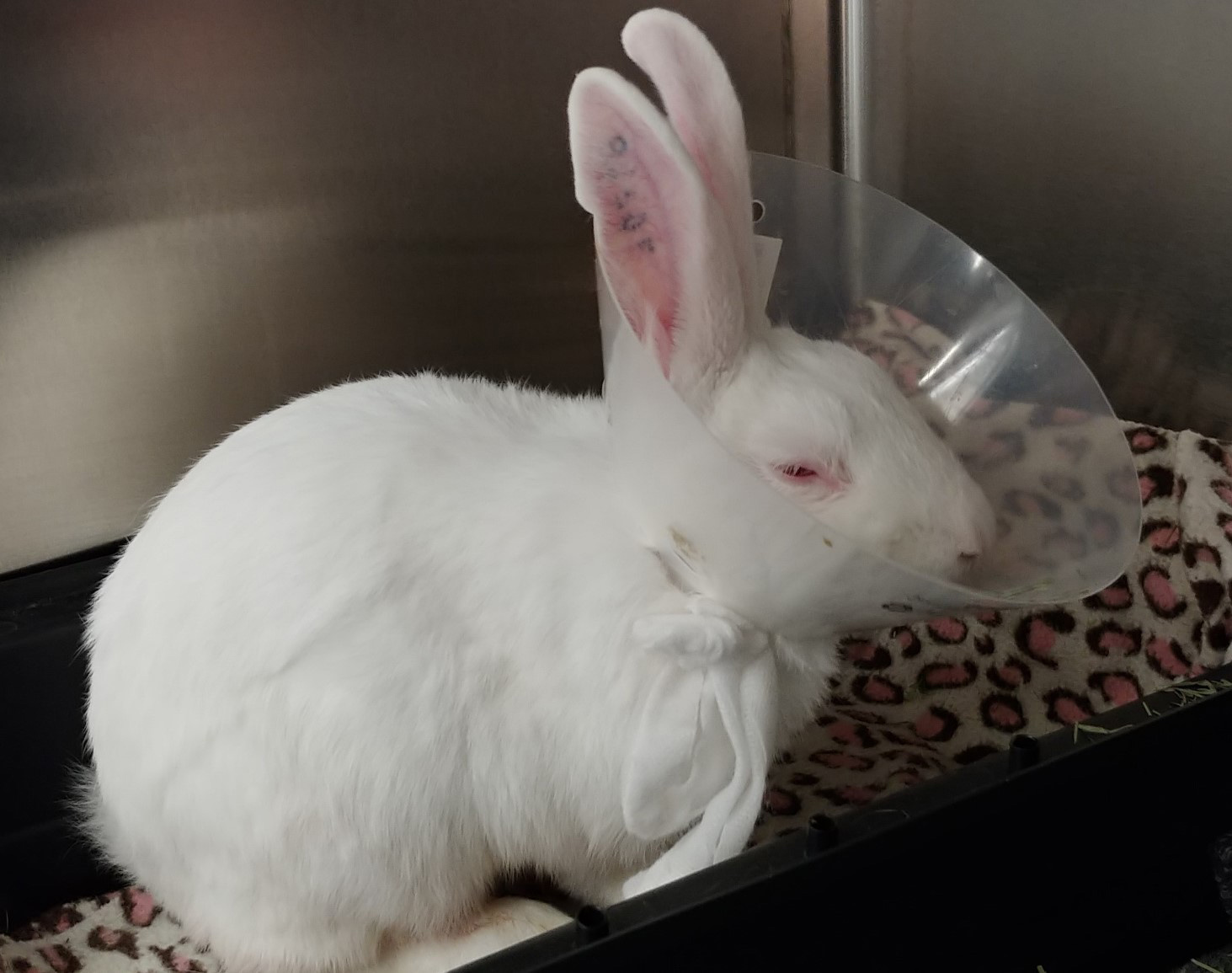
This is a severely painful rabbit. The orbits are tightened, the nostril is in a V-shape, the cheeks are flat, there is a hunched posture and if not for the e-collar the ears would be flattened and backwards.
What testing should be offered?
It should be obvious by the variety of potential conditions that cause GI stasis, that individual cases can be unique in the diagnostic needs; however, there are some universals. A systematic, thorough physical examination should always be conducted. While at rest, a pain evaluation should be conducted as objectively as possible. I recommend becoming familiar with the Rabbit Grimace Scale, an objective measure of pain in rabbits: https://www.nc3rs.org.uk/rabbit-grimace-scale. Thoracic auscultation should be performed to assess the heart and lungs. In addition, it’s important to auscultate the abdomen for borborygmi (one of my favorite medical words). Under normal conditions you should be able to hear at least 3-4 good sounds per minute. Hypo-or hyper-motility can both indicate problems. Abdominal palpation can reveal masses, gas distention of the stomach, small intestine or cecum and can show areas of pain. If stable enough, a dental examination should be performed. If one is not performed, then follow-up should be arranged to include a dental examination as soon as possible.
Abdominal radiographs are always wise for cases of GI stasis. The stomach is well protected by the ribs in these animals and there can be a fair degree of pathology that may not be detected on palpation. For a correct diagnosis, prognosis and formation of a treatment plan, there is little that gets more information for the cost and effort in most of these cases than the abdominal radiographs.

Placement radiograph for a naso-gastric tube. When advanced into the stomach, it can be used for periodically removing gas or fluid in the case of gastric distention. Once the obstruction is clearing, the same tube can be used to start slowly trickle feeding.
Basic bloodwork can also have a very high yield. Renal values, packed cell volume and electrolytes can give objective measure of hydration. Liver values can help identify liver lobe torsion, a growing problem in many rabbit breeds. Blood glucose can be of prognostic value in rabbits with GI stasis. Values over 350 mg/dL are associated with a worse outcome. However, I would caution against over-interpretation. Being aware of a significant elevation and trending response is a far more reliable prognostic indicator than a single value. I try hard to never doom a patient based on the blood glucose, but I do use it to help decide how aggressive the supportive care plan should be. By contrast, lactate is highly variable in herbivores and does not have the prognostic value it does in other domestic species. Don’t let an elevation scare you too much.
A complete blood count can be of some value. Look at the white cell count and look for toxic changes to guide judicious use of antibiotic medication. Antibiotics are not frequently indicated for stasis cases, but they are important when needed. When not indicated, they can add to feelings of nausea and potentially put further stress on the normal flora, so avoiding them when not indicated is not only responsible medicine, but good for the individual patient. Sometimes even a brief look at a blood smear helps give enough to guide these decisions.
Finally, an ultrasound can be a good follow-up tool to fine tune information gained from radiographs and blood testing. These species do have large ceca that are generally gas-filled, but with a little patience and practice, you can still get diagnostic images of the liver, kidneys, stomach, duodenum, jejunum and urinary bladder.
When does an animal need inpatient care?
Looking through the indications for inpatient care that guide my practice and what is supported in literature, I have found three broad categories that I find serve to be good guides:
- Signs of shock
- Any uncontrolled pain
- Obstructive signs
There is some overlap in the categories, but that helps reinforce and provide a safety net so that none are missed.
Signs of shock may be detected on physical examination and diagnostic testing. On physical examination you may see tachycardia, delayed capillary refill time, and alterations in mental status. The mental status alterations may be seen as a dull mentation or just a frozen stance characteristic of a prey animal experiencing stress or fear. Of course this can happen with a different environment, but often I will quiz the owners or have them comment about how the behavior is different from other hospital visits. Radiographs may show microcardia. Blood testing may show increases in PCV/TP. Any change to BUN is significant, as small herbivores have a slower rise in BUN than omnivores or carnivores. Finally, hyperglycemia should be considered as a likely sign of shock and be something that reinforces a decision to treat more aggressively.
Uncontrolled pain is another reason to hospitalize. The two most common underlying processes in stasis are dehydration (see shock above) and pain. Correcting these two issues can make the difference between medical and surgical management, success and failure, life and death. Utilizing the Rabbit Grimace Scale and seeing reaction to palpation can give an objective measure of pain. A grimace scale score over 4-5 is unlikely to be corrected with outpatient medication. If I have doubt, I will often give a single dose of Buprenorphine as an intramuscular injection and wait 30 minutes. If there is not a substantial improvement in the grimace scale score, then hospitalization is indicated. Along with the hospitalization, more importance should be placed on diagnostic testing to determine the underlying cause, as some of the causes of more significant pain may require specialized care, like surgery for liver lobe torsion.

There is severe fluid distention of the stomach, a clear indication of pyloric obstruction. This is a definite indication for inpatient care and may require surgery.
Obstructive signs are always an indication for inpatient care. Many cases of GI stasis are the result of an obstruction in the GI tract. Obstruction is very serious in these animals and can result in the need for surgery. However, with aggressive inpatient care they can often be resolved medically. Most of the obstructions are the result of furballs or fiber mats and are properly viewed as “mobile obstructions” that will move through the intestine with adequate hydration and pain control. If surgery is needed, the initial inpatient treatment will help stabilize the patient and increase the likelihood of a good outcome. On physical examination, hypermotility is often detected at the onset of an obstruction. The intestine starts moving faster to try to push through the obstruction. As time goes on, this shifts to hypomotility or complete absence of digestive sounds. Gastric distension may be palpated or seen on radiographs. Distention, be it fluid or gas, in the stomach is far more significant in herbivores. They are unable to eructate to clear the gas and their stomachs are designed for grazing. Any distention can be very painful and can have significant impact on perfusion of the stomach. Rapid resolution is imperative to successful treatment.
What can be expected with inpatient care?
Inpatient care allows for more definitive treatment of all the indicators listed above. Shock and dehydration are helped profoundly with IV fluids. Just as with dogs and cats, more than mild dehydration should be treated with IV fluids. Vascular collapse from shock is also best treated with IV fluids: usually crystalloids, but sometimes colloids or hypertonic saline. Far better pain control is available to inpatients. Oral pain medication in small herbivores is generally limited to meloxicam. Gabapentin, transmucosal buprenorphine and oral Tramadol have questionable efficacy in these species. Along with IV fluids, pain CRIs can be utilized to allow very effective analgesia that can be fine-tuned for the individual. Maropitant is a good adjunct for visceral pain. If obstruction is present and gastric distention is present, decompression can be achieved by passage of an oro-gastric tube or placement of a naso-gastric tube. If surgery is ultimately indicated, Bulger has a state-of-the-art facility and a highly trained staff ready to offer the best care possible.
Serial radiographs, blood testing and ultrasound monitoring can help guide treatment 24 hours a day, avoiding delays that could cause serious lapses in treatment.
Given the seriousness of the conditions, we have a very good success rate at Bulger and manage to resolve the majority of treatable stasis cases, usually with aggressive medical care. We are here to help you and happy to offer any consultation that may help you with outpatient care or help decide when inpatient care is needed.